Supraventricular tachycardia (SVT) is a cardiac arrhythmia associated with a rapid and very regular rate, which can reach 180 to 220 beats per minute, and which does not originate from the cardiac conductor, the sinus node.
Its starting point is located above the ventricles
This arrhythmia originates from regions above the ventricles, hence its name: supraventricular.
A Brief Review of Heart Anatomy
The heart is composed of four chambers.
The upper part consists of the right and left atriaThe atria are the two upper chambers of the heart. They act as reservoirs for blood that will fill the ventricles. (RA-LA), while the lower part consists of the right and left ventricles (RV-LV).
This organ is the engine of life, and its four chambers act as reservoirs for bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood. When the heart contracts, it pumps and propels bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood throughout the body.
To function properly, this pump needs an electrical impulse to determine the number of beats per minute.
The Cardiac Electrical System
The heart’s electrical system generates this impulse, and its various components are responsible for synchronizing the heart’s contraction efficiently, from bottom to top.
Like a House's Electrical System
The heart has an electrical network, similar to that of a house. It is constructed as follows:
The current arrives at the second floor where the electrical generator is located.
The current then passes to the first floor through a single point; this is where the control box is located.
From this control box, the current is directed to the lower rooms via specialized, high-conduction wires.
Reviewing It from a Cardiac Perspective
The conductor of this electrical system is located at the top of the heart, in the right atrium. It is a cluster of cells called the sinoatrial node, which is actually the heart’s natural pacemaker. It initiates all heartbeats and determines the heart rate.
This heart rate, or cardiac rhythm, is called the sinus rhythm because of its starting point, the sinoatrial node.
An Organized Electrical Transmission
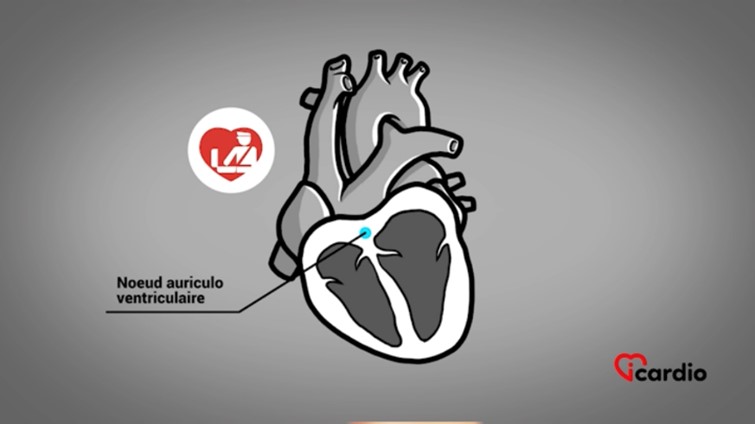
The electricity generated by this node is transmitted to the atria and ventricles through the only possible pathway, the electrical customs officer, known as the atrioventricular (AV) node. This “customs officer” controls the speed of the electrical passage.
Following this mandatory passage, the electricity reaches the ventricles through a fast conduction network called the Purkinje fibers.
Normal Heart Rate
A normal heart rate is considered to be between 60 and 100 beats per minute.
It Varies Throughout the Day
It is normal for the heart rate to vary throughout the day. The heart beats more slowly when at rest, partly due to the effect of certain medications, and speeds up during physical activity or stress, for example.
There is a Short Circuit in the Electrical Network
The underlying problem with supraventricular tachycardia (SVT) is that it is, in a way, an electrical short circuit in the heart’s electrical network. As a result, the heart beats rapidly even when the person is at rest, without any external stimulation.
It Goes Fast!
The typical heart rate for this type of arrhythmia is between 140 and 220 beats per minute, very regular.
Who is Affected?
SVTs can affect both children and adults of all ages, often those in good health.
This anomaly is not hereditary and is unrelated to the presence or absence of blocked coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that.
What Are the Symptoms?
This arrhythmia usually manifests as the sudden onset of palpitations, a “racing heart” sensation, and ends abruptly with the return to sinus rhythm, the normal heart rhythm.
It can feel like engaging in intense physical activity, with the heart pounding and seeming to want to burst out of the chest, even while at rest.
A Classic Comparison
The onset and end of palpitations“Palpitation” is a symptom related to an abnormality in heartbeats. There are several types of arrhythmias. This term is like a surname that encompasses several first names. can be compared to switching a light on and off. For example, the heart rate can suddenly jump from 80 to 180 beats per minute, then abruptly return to 80 beats per minute.
This description of the sudden start and end of the palpitations“Palpitation” is a symptom related to an abnormality in heartbeats. There are several types of arrhythmias. This term is like a surname that encompasses several first names. episode immediately guides the healthcare professional toward a diagnosis of SVT.
Variable Duration
An SVT can be short-lived, lasting just a few minutes. It can also sometimes last for a few hours, or even several hours, occasionally forcing the person to go to the emergency room to receive intravenous treatment to stop the episode.
Other Possible Discomforts
Some people do not perceive palpitations“Palpitation” is a symptom related to an abnormality in heartbeats. There are several types of arrhythmias. This term is like a surname that encompasses several first names. as rapid beats but instead experience sudden shortness of breath, chest pain, or dizziness. These symptoms are caused by the high and sustained heart rate.
Not Life-Threatening, But Disruptive
SVT is not fatal or dangerous.
However, it affects the quality of life as it can occur at any time, day or night, without any precipitating or predisposing factors.
Highly Variable Frequency
The frequency of episodes varies from one individual to another and can change over time in the same person.
Indeed, episodes can occur once a year or two to three times a week. Unfortunately, the frequency is not fixed.
Repeated episodes of SVT can occur during adolescence, followed by a calm period lasting several years, with a recurrence during menopause or andropause.
The Why and How
Three main mechanisms are primarily responsible for SVT:
Short Circuit in the Electrical Customs Officer: Called nodal reentry (50 to 70% of cases).
An Extra Electrical Pathway in the Heart Present from Birth: Known as an accessory electrical pathway (20 to 30% of cases).
Short Circuit in the Atrium: Called paroxysmal atrial tachycardia (PAT) (10 to 20% of cases).
• Nodal Reentry
In about 30% of the population, the region of the electrical customs officer, or the atrioventricular (AV) node region, consists of two electrical pathways. There is a slow conduction pathway and a fast conduction pathway of the AV node; this is a normal variant.
As long as the electricity passes through both electrical pathways simultaneously, the electrical signal reaches the ventricles at the same time and does not cause any short circuits, thus no arrhythmia.
SVT by nodal reentry can be triggered by the premature production of electricity called an extrasystole. An extrasystole is produced either at the atrium (atrial extrasystole or AES) or at the ventricle (ventricular extrasystole or VES).
It is most often asymptomatic or felt in different forms depending on the individual. Some describe it as a pause in the heart or a more vigorous beat.
If the extrasystole enters the AV node by passing equally or synchronously through the slow and fast pathways, there will be no short circuit. However, if the extrasystole arrives at a precise moment when one of the two electrical pathways is not ready to let the current pass, the electricity will only descend through one pathway and travel the other in reverse, creating a microelectrical circle that results in paroxysmal supraventricular tachycardia (PSVT).
• Accessory Pathway (Formerly Called Wolff-Parkinson-White)
An accessory pathway is an additional electrical wire present from birth that connects the atrium to the ventricle. This electrical wire bypasses the control of the AV node. It can be located on the right or left side of the heart.
In some cases, this pathway is inconsequential and will never cause arrhythmia.
However, in other cases, the trigger for SVT by an accessory pathway is, once again, extrasystoles.
When triggered, the electrical activity descends through the AV node and ascends retrogradely through the accessory pathway. The electrical activity is then ready to descend to the ventricle through the AV node again, creating an electrical circuit. This loop can also occur in the opposite direction, descending into the ventricle through the accessory pathway and ascending through the AV node.
• Paroxysmal Atrial Tachycardia (PAT)
Paroxysmal atrial tachycardia can originate from the right atrium or the left atrium. A microelectrical circle forms there, taking over from the heart’s natural conductor and producing very rapid electricity, thus causing SVT.
Treatment
The treatment of SVT varies from one individual to another. It is directly related to the frequency of episodes, their duration, the symptoms experienced, and the impact on the person’s quality of life.
Tricks to Try
Valsalva maneuvers can sometimes stop supraventricular tachycardia (SVT).
Straining the Abdomen: This maneuver involves straining as if having a difficult bowel movement.
Cooling the Face: Another maneuver involves quickly placing a cold towel on the face or submerging the face in a bucket of ice water.
These interventions can affect the heart’s nerve connections and influence its electrical system, returning it to its normal rate.
Therapy
Several therapies can be used depending on the symptoms, the frequency of arrhythmias, their duration, and their recurrence.
A "Just in Case" Prescription
If an episode occurs and the Valsalva maneuver proves ineffective, medication would then be prescribed to the patient. The medication, taken as a pill at that time, can stop the arrhythmia.
More Specific Medication
When episodes are frequent and affect a person’s quality of life, doctors may prescribe medication that slows down the electrical conduction at the level of the electrical customs officer, the AV node.
In other cases, different medication acting specifically on the atrial electrical activity or the accessory pathway may be used.
The effectiveness of the medication varies greatly. Additionally, even if it is effective, the medication can sometimes cause side effects that may lead to a change in treatment or, simply, discontinuation of it.
A Definitive Therapy: Ablation
Another method to definitively eliminate SVTs is catheter ablation. This treatment cures SVT by destroying the area responsible for the arrhythmia.
Electrophysiological Study
The first step of this treatment is to conduct an electrophysiological study (EPS), which involves studying the heart’s electrical activity to identify the mechanism of the SVT.
This examination is performed using catheters that are inserted into the veins of the body and guided to different areas of the heart.
Ablation
These catheters record the heart’s electrical signals. This allows specialists to precisely locate the SVT and destroy the short circuit. This procedure is carried out using a catheter that burns the area, either by heat (radiofrequency) or by cold (cryoablation).
Duration of the Procedure
The duration of the procedure varies. Typically, a maximum of 2 hours is sufficient to perform the intervention.
Excellent Success Rates
Success rates vary depending on the mechanisms of the SVT; however, they are generally high, reaching 95% in most cases.
Risks Associated with the Procedure
As with any surgical intervention, ablation carries risks.
Major complications related to the procedure occur in ≤ 1% of cases (requiring a pacemaker implantation, heart attack, cardiac perforation, etc.).
Minor complications can occur, such as slight bleeding or the formation of a hematoma (bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood collection at the catheter insertion sites).
Reminder
It is important to remember that the treatment chosen for SVT varies from one individual to another. The different advantages and risks of each option are presented by the healthcare professional.
The final decision rests with the patient, after discussion with their treating physician.