Spontaneous Coronary Artery Dissection (SCAD)
- Home
- »
- Coronary heart diseases
- »
- Spontaneous Coronary Artery Dissection (SCAD)

The heart is an extraordinary muscular pump that ensures bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood circulation throughout the body. It is the engine of life.
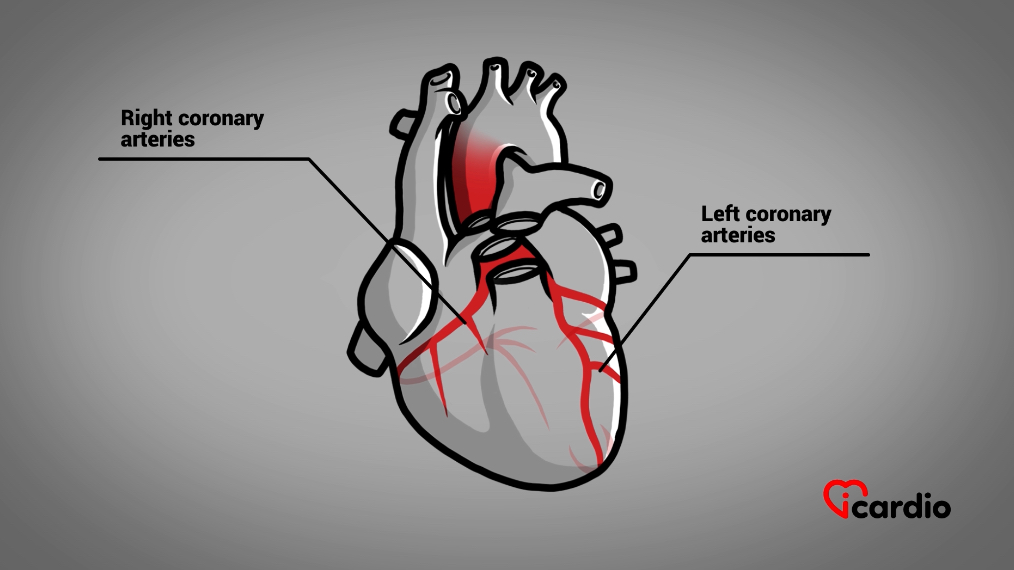
The coronary arteries
This muscle, the heart, uses oxygen delivered to it by “pipes” called coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that. These arteries run over the heart and penetrate it, supplying oxygen-rich bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood. The diameter of the arteries varies between 2 and 4 mm.
Any disease that alters their diameter can compromise the heart’s functions and sometimes affect it permanently.
Components of an Artery
There are two main coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that that supply bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood to the heart. These two arteries, along with all other coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that, are composed of three layers: the intima, the media, and the adventitia.
Each of these layers has a specific role.

Internal layer: intima
The inner wall, called the intima, is comparable to a thin layer of Teflon.
It is responsible for keeping the vessel in good condition and protecting it against the formation of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood clots.
Middle layer: media
Located between the other two layers, the media is thicker and contains smooth muscle cells.
The media allows the artery to contract and then dilate.
External layer: adventitia
The adventitia is the outermost layer. It is the strongest part of the artery, and its role is to protect the vessel.

Three Main Types of Obstacles
Coronary circulation can be impeded in three ways, all originating from the muscular layer of the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessel, the media:
1-Coronary Artery Spasm:
This can occur spontaneously or be triggered by the consumption of substances such as cocaine. A coronary spasm is a contraction of the muscular layer of the media, which effectively chokes the vessel.
The severity of the consequences of this constriction depends on the extent of the spasm—whether it causes a complete or partial closure of the artery—and the duration of the spasm.

2-Spontaneous Dissection or Tear of the Media:
The exact cause of this is not well understood, but it is believed to be associated with an abnormality in the media.
The consequences will again depend on the severity of the internal tear in the vessel and whether it causes a partial or total blockage of the artery.

3-Rupture of an Atheromatous Plaque:
More commonly referred to as a rupture of a cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaque, this is by far the most common cause of impaired coronary circulation.

Let’s take a closer look at arterial dissection or spontaneous tear of the media.
What is a Spontaneous Coronary Artery Dissection (SCAD)?
A SCAD, as the name suggests, is a tear in the wall of a coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that that occurs suddenly, without an identified cause.
A Tear Occurs
A rupture can occur and be localized solely within the muscular layer, thus confined to the inside of the coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that wall. This dissection causes bleeding within the media.
Depending on the extent of the bleeding, a bulge will form inside the vessel, leading to either partial or complete obstruction of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow.
In some cases, the dissection may also involve the thin inner layer of the vessel, the intima. If this happens, bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow could infiltrate and further tear the vessel wall.

And as if that weren't enough!
Another process can exacerbate SCAD: the addition of a thrombus, or more precisely, the development of a blood clot at the site of the arterial tear.
When the artery wall tears and exposes its inner components, the body initiates a process to seal the breach, leading to the formation of a bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood clot. This process begins with the activation of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood plateletsPlatelets, also known as thrombocytes, are small cell fragments produced by the bone marrow. They play a crucial role in blood clotting by forming aggregates and clots to stop bleeding when blood vessels are damaged. >>.
The Alarm Has Sounded for Blood Platelets
PlateletsPlatelets, also known as thrombocytes, are small cell fragments produced by the bone marrow. They play a crucial role in blood clotting by forming aggregates and clots to stop bleeding when blood vessels are damaged. >> are small particles found in the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood. More precisely, they are tiny fragments of large cells contained in the bone marrow.
They play an important role in bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood coagulation, the process by which bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood transitions from a liquid state to a gel to form a clot.

Understanding Blood Coagulation
When we get a cut, the wound bleeds. BloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flows because there is a breach in the blood vessels. The body sends out an alarm signal, as it needs to cover or close the breach. This is where bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood coagulation comes into play.

Clot Formation
Thrombocytes, or bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood platelets, are the first cells to spring into action. Upon contact with the elements beneath the thin layer of the vessel known as the intima, they change shape, produce tentacles, and clump together. They form the primary structure of the clot.
PlateletsPlatelets, also known as thrombocytes, are small cell fragments produced by the bone marrow. They play a crucial role in blood clotting by forming aggregates and clots to stop bleeding when blood vessels are damaged. >> also release substances that attract more plateletsPlatelets, also known as thrombocytes, are small cell fragments produced by the bone marrow. They play a crucial role in blood clotting by forming aggregates and clots to stop bleeding when blood vessels are damaged. >> and initiate the next steps of the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood coagulation process by transforming certain bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood proteinsProteins are fundamental components manufactured by the cells of our body. They play an essential role in many biological functions, acting as hormones, antibodies, and even cholesterol transporters, among others. >> into tiny filaments.
The accumulation of these filaments around the plateletsPlatelets, also known as thrombocytes, are small cell fragments produced by the bone marrow. They play a crucial role in blood clotting by forming aggregates and clots to stop bleeding when blood vessels are damaged. >> and trapped red bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood cells creates a mesh that further solidifies and seals the clot.
Partial or Complete Obstruction
Whether the tear is confined to the inside of the coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that wall or includes the intima, the accumulation of blood in the arterial wall, with or without the formation of a clot in a coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that, can lead to one of two situations: partial or complete obstruction of the vessel.
Clinically, these conditions can result in a non-ST elevation myocardial infarction (NSTEMI) or an ST elevation myocardial infarction (STEMI).
Who is at Risk?
According to medical records, approximately 1 to 4% of myocardial infarctions and 0.5% of cardiac arrests are caused by Spontaneous Coronary ArteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that Dissection (SCAD).
In nearly 90% of cases, the victims are women aged 40 to 55 years.
What are the Potential Causes and Risk Factors of SCAD?
SCAD is not caused by atherosclerotic plaques (atherosclerosis). The exact origin of this condition is still unknown. In more than 20% of cases, the cause remains unidentified.

It is important to consider the following as predisposing factors:
- Certain connective tissue disorders involving elements between the cells, such as Marfan syndrome and Ehlers-Danlos syndrome, among others.
- Hereditary factors have been suggested. Certain genetic mutations are currently under study.
- Estrogen hormone therapy is also suspected, although no clinical evidence has been found to date.
In patients with fragile arteries, dissection can be triggered by:
- Emotional or physical stress,
- Intense physical activity,
- The use of stimulants, such as cocaine,
- Childbirth and pregnancy.

It is important to consider the following as predisposing factors:
- Certain connective tissue disorders involving elements between the cells, such as Marfan syndrome and Ehlers-Danlos syndrome, among others.
- Hereditary factors have been suggested. Certain genetic mutations are currently under study.
- Estrogen hormone therapy is also suspected, although no clinical evidence has been found to date.
In patients with fragile arteries, dissection can be triggered by:
- Emotional or physical stress,
- Intense physical activity,
- The use of stimulants, such as cocaine,
- Childbirth and pregnancy.
What are the Symptoms?
The symptoms of Spontaneous Coronary ArteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that Dissection (SCAD) are quite similar to those experienced during a lesion caused by the rupture of a cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaque.
The sudden onset of chest pain can be described as discomfort or tightness in the chest area, with or without radiation to:
- the neck,
- the jaw,
- the left arm.
It can also lead to arrhythmia or cardiac arrest.

Why Similar Symptoms?
The set of symptoms that characterize a coronary event due to the rupture of a cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaque (Acute Coronary Syndrome or ACS) and SCAD are very similar because they share the same origin: a restriction or blockage of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow.
It is understandable that there may be some hesitation in making a diagnosis due to the close similarity between the symptoms of these two conditions.
How to Make a Diagnosis?
A SCAD may be suspected in a patient presenting with a heart attack if:
- They show no risk factors for atherosclerotic coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease,
- They are under 50 years old,
- They have experienced significant physical or emotional stress,
- They have health issues that predispose them to SCAD.
Variations or changes can be seen on an electrocardiogram (ECG) and sometimes even on an echocardiogram using ultrasound.
As for bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood tests, the levels of proteinsProteins are fundamental components manufactured by the cells of our body. They play an essential role in many biological functions, acting as hormones, antibodies, and even cholesterol transporters, among others. >> released by the damaged heart muscle (troponins) will also be elevated. However, a definitive diagnosis can only be made through coronary angiography, which allows the specialist to directly visualize the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that.

How is SCAD Treated?
Doctors often favor a conservative approach, meaning they opt to observe the clinical evolution of the situation, as arteries tend to heal on their own over time.
To clarify, conservative treatment is a medical approach where the main idea is to avoid subjecting the patient to invasive measures, such as catheter interventions.
It is recommended to avoid the use of stents in treating an artery because the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessels are fragile, and there is a risk of worsening the dissection by causing it to extend further.
Medications are given to slow the heart rate and lower bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood pressure to aid the healing process. An antiplatelet agent may be used, but so far, no clinical benefit has been demonstrated.
If symptoms persist despite conservative treatment or if the patient’s condition worsens, coronary angioplasty, with or without stents, may be attempted. However, the success of this procedure is mixed, as some arterial tears can be quite extensive.
It is very rare to require heart surgery, though it may be necessary in some cases.
In general, complete healing of the coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that is expected within 3 months for 95% of patients.

What Tests Can Be Expected?
In the presence of chest pain, the basic tests usually include:
- Blood Tests: To detect markers of cardiac stress, such as troponin.
- Electrocardiogram (ECG): To assess the electrical activity of the heart and identify abnormalities that may indicate ischemia or a heart attack.
- Chest X-ray: To examine the lungs and heart, ruling out other causes of chest pain, such as pneumonia or pleural effusion.
- Transthoracic Echocardiography: This test visualizes the impact of the dissection on the heart’s muscle function.
- Coronary Angiography: The reference test to confirm the diagnosis, highlighting the rupture of the coronary wall and its impact on bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow.
- CT Scan: Recent medical reviews also suggest the necessity of a CT scan of the neck, chest, and abdomen to screen for potential fibromuscular dysplasia, an abnormality of the vessel’s muscular layer.

Can a Dissection Recur?
In the most advanced studies on SCAD, a recurrence has been reported in less than 3% of patients over a 3-year period.
This underscores the importance of following medical advice when a case of Spontaneous Coronary ArteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that Dissection occurs.
What Should Be Done After Experiencing a Spontaneous Dissection?
Maintain Normal to Low Blood Pressure: Keeping blood pressure in a lower range helps reduce the stress on the arteries.
Prescription of Beta-Blockers: These medications are prescribed to reduce the shear stress on the patient’s arteries, meaning the workload that bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow imposes on the arteries with each heartbeat.
Engage in Moderate-Intensity Exercise: It is recommended to limit weight lifting to 30 lbs for women and 50 lbs for men. Additionally, it is suggested to avoid pregnancy, as SCAD can recur in 14% of cases in women who have previously experienced it, according to secondary studies.
It is also suggested to avoid pregnancy, as SCAD can recur in 14% of cases in patients who have previously experienced it, according to secondary studies.
Participate in a Cardiac Rehabilitation Program: This program is considered beneficial as it allows the patient to safely begin light to moderate exercise.
Join a Psychological Support Program: Psychological support is recommended if the patient feels the need, as SCAD can be a traumatic experience.

Driving
Driving a vehicle after a cardiac event depends on the extent of the heart damage and the type of driver involved. The patient should discuss this with their doctor. In some provinces, the guidelines are as follows:
STEMI:
- After a STEMI-type heart attack, driving is subject to certain restrictions. Generally, a patient should wait 1 month after the event before resuming driving.
- For commercial drivers (bus, truck, and other similar vehicle operators), the waiting period is extended to 3 months from the date the patient was discharged from the hospital.
NSTEMI:
- For a less severe heart attack, such as NSTEMI, which only required observation and non-urgent surgical intervention, driving can be resumed 48 hours after the cardiac procedure. However, an echocardiographic study confirming only minimal heart damage is required.
- For commercial driving, the patient must wait up to 7 days before getting back behind the wheel. There are various other recommendations depending on the situation; for example, a minor heart attack without major severity, no arterial intervention, or complications related to valves or arrhythmias, and so on.

In these specific cases, it is wise for the patient to consult their cardiologist for an informed opinion on the appropriate waiting period before resuming driving.
Doctors do not automatically report to the provincial driving authority (such as the SAAQ in Quebec) that a patient has suffered a stroke or other cardiac event. It depends on the patient’s willingness to follow the medical directives given to them.
Such is the law in several Canadian provinces.
However, if the patient were unfortunate enough to cause an accident due to a symptom or cardiac complication during the period when they were advised not to drive, they could be held fully responsible for the outcome of the accident, having endangered their own life and the lives of others.
What Follow-Up is Recommended?
After a SCAD, ongoing medical follow-up with a healthcare professional is essential.
Long-term follow-up with a cardiologist is fully justified since this is a relatively recent condition, and the medical community still has much to learn about it.
The frequency of appointments will depend on the timing and severity of the event.

Related articles



Latest articles





