The heart, located in the center of the chest between the two lungs, is an essential muscular pump that acts as the engine for bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood circulation.
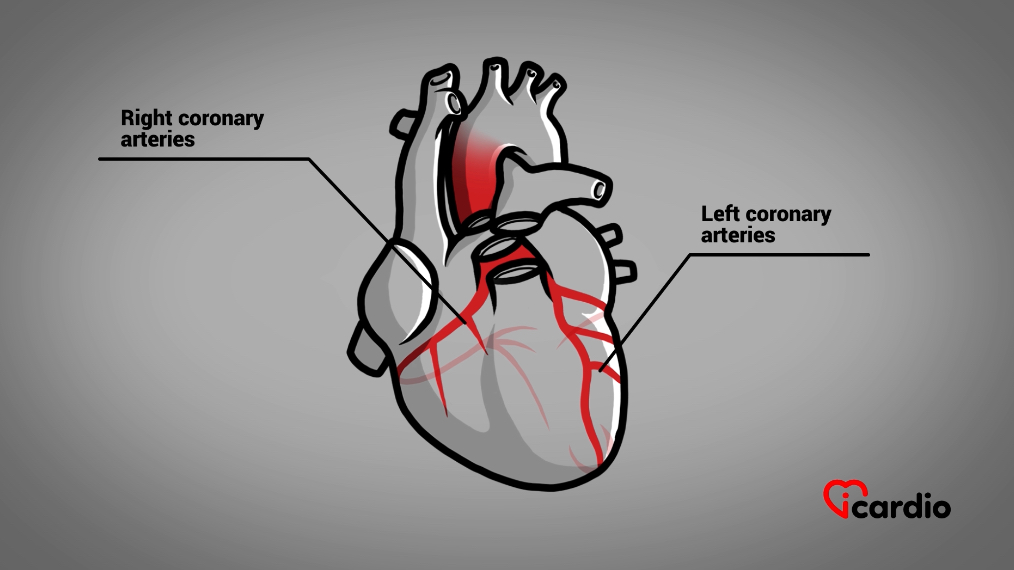
The proper functioning of the heart muscle depends directly on its oxygenation, a task ensured by two main arteries: the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that.
Oxygenation of the Heart and Its Arteries
The right and left coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that originate at the root of the aorta and then move toward the heart. They branch out into several smaller arteries to ensure the entire heart muscle is supplied with bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood. These branches further divide into fine arterioles that travel through the heart muscle and eventually extend into capillaries.
At this point, the red bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood cells release the oxygen needed for the heart to function properly and collect carbon dioxide, just as they do throughout the body.
Four Determinants of the Heart’s Oxygen Needs
The heart’s oxygen needs are influenced by several factors: the amount of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood filling the left ventricle, the resistance to bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood ejection, the strength of the heart muscle’s contraction, and the heart rate.
Oxygen Transport and Blood Vessels
The supply of oxygen is primarily determined by the number of red bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood cells in the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood and the condition of the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessels that deliver oxygen to the heart muscle cells.
These vessels are composed of three layers
BloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessels consist of three layers, each with a specific function. However, it is the middle layer that is particularly involved in the development of cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaques.
• Inner Layer: Intima
The inner layer, called the intima, acts as a thin protective membrane, similar to a layer of Teflon. It maintains the health of the vessel and protects it from the formation of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood clots.
The intima naturally secretes substances that dilate the vessel when necessary and “lubricate” it, preventing harmful substances from adhering to the walls. One of these substances functions similarly to nitroglycerin, which some patients use to relieve angina. In this way, the intima helps dilate vessels when needed.
• Middle Layer: Media
The middle layer, or media, is thicker and composed of muscle cells. It enables the artery to contract, spasm, or dilate.
Nitroglycerin, used to relieve chest pain (angina), acts directly on this layer, relaxing it and allowing the vessels to expand, thereby increasing bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow and relieving angina.
This is also the layer where cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaques form, giving arteries a yellowish appearance when viewed from the inside.
• Outer Layer: Adventitia
The adventitia forms the outermost layer of the vessel. It is the toughest part, providing additional protection to the artery.
Arterial pollutants
Major pollutants, such as tobacco products and cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, can harm the health of arteries and lead to serious diseases.
The infamous cholesterol
We often hear about “bad” cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, the kind that clogs arteries, but few people know that cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plays a vital role in the human body.
Necessary for life
CholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> is actually present in every cell of the body. It is essential for the integrity and proper functioning of cell membranes—the outer layer of cells.
It also contributes to hormone production, plays a role in the immune system’s defense against infections, and helps digest fats through bile salts.
Vital, but with a dangerous side
So, how can something so essential also be harmful?
It all comes down to balance and the amount of cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> present in the blood.
We all produce it
Every day, our body produces cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> in the liver. This type of cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, called endogenous, is naturally made by our own bodies.
We have a biological “thermostat” that regulates its production, a process that is genetically determined and varies from person to person.
We all consume it
Exogenous cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, on the other hand, comes from our diet. It is absorbed by the intestine and directed to the liver, where it is integrated into our circulatory system.
Needs a transporter in the blood
Since cholesterol is a fatty molecule, it does not dissolve in the blood. Whether it comes from food or is produced by the body, it requires “transporters,” or “taxis,” to move through the bloodstream.
The good “taxi,” also known as good cholesterol, is HDL, while the bad “taxi,” or bad cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, is LDL.
Bad and Good Cholesterol
LDL, or bad cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, carries cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> from the liver to the cells of the body.
When the cells don’t need all the cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> being transported, the excess is brought back to the liver by HDL, or good cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>.
This excess cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> is then eliminated by the gallbladder in the form of bile salts, which are essential for the digestion of fats.
Cholesterol Imprint in the Artery
From birth, the transport of cholesterol begins to leave traces on the walls of our arteries.
Over time and with aging, these deposits accumulate and thicken, gradually forming plaques in the arterial walls.
Formation of Cholesterol Plaques
The formation of atherosclerotic plaques begins with the deposit of bad cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> (LDL) on the thin inner layer of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessels, called the intima.
It is then absorbed and accumulates in the muscular layer of the vessel wall, the media, where it triggers an inflammatory response.
Macrophage cells, responsible for cleaning the body, attempt to “eat” this cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>. As they fill up with cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >>, they become trapped in the vessel wall, forming foam cells loaded with fat. When these cells die, they release their contents, further increasing inflammation, perpetuating the cycle of deposition and inflammation.
Where does excess bad cholesterol come from?
Excess bad cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> (LDL) can come from several sources:
Poor dietary habits, particularly a high intake of saturated fats;
Genetic predispositions, meaning a family inheritance;
Certain medical conditions, such as kidney or thyroid disorders.
Atherosclerotic Plaques
The number and size of atherosclerotic plaques vary depending on the amount of excess LDL cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> in the body, as well as the presence of genetic predispositions.
Excess bad cholesterol (LDL) plays a key role in the development and size of plaques. Additionally, some individuals, due to genetic factors or other predispositions, are more prone to developing these plaques than others.
LDL "Taxi" Parts Also Pollute
The “taxis” of bad cholesterol (LDL) also play a role in the formation of atherosclerotic plaques.
Just like the pollution caused by cars on the road, certain proteins in the composition of LDL “taxis,” known as apoproteins, contribute to the inflammation of arterial walls.
Researchers are currently focusing on these proteinsProteins are fundamental components manufactured by the cells of our body. They play an essential role in many biological functions, acting as hormones, antibodies, and even cholesterol transporters, among others. >>, hoping to develop medications that can reduce their presence, potentially leading to improved cardiovascular health.
Small Plaques Have No Effect on Oxygen Supply
Most small plaques that develop over time in the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that do not alter bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow or the oxygen supply to the heart muscle.
They Can Affect the Artery’s Muscle Layer
However, in some cases, the presence of plaques can cause deformations in the blood vessels.
Though rare, these deformations can, in very slight cases, lead to the formation of aneurysms.
Formation d’anévrismes possible
An aneurysm is characterized by a weakening of the artery’s muscle layer, making it less resistant.
This weakness, combined with internal vessel pressure, causes a localized deformation and dilation. Fortunately, the rupture of an aneurysm in the heart is extremely rare.
An aneurysm can be compared to a bulge on a garden hose, where internal pressure creates a weak point and expansion.
The Plaque Takes Up Space in the Wall and Organizes Itself
The accumulation of cells and fatty substances in the arterial wall causes the intima, the inner layer of the vessel, to lift. Like a pimple, the surface of the plaque becomes stretched and fragile.
The inflammation caused by cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> in the wall activates the body’s natural repair mechanisms, leading to the formation of fibrous tissue—a tough, white structure similar to that found in meat. This fibrosis makes the plaque more rigid, firm, and stable.
Over time, calcium deposits may also form, further reinforcing the plaque.
An Artery Is Always Moving, Especially Around the Heart
Blood vessels expand and contract with every heartbeat. You can feel this movement by checking your pulse at the neck or wrist. Coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that not only undergo this regular stretching but are also constantly affected by the heart’s continuous motion.
With this incessant movement, a cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaque can spontaneously rupture. Regardless of their size, it’s often the more fragile and brittle plaques that are prone to cracking, leading to acute coronary events like unstable angina or a heart attack.
Beware of Intense Efforts
This phenomenon may explain why certain plaques rupture during sudden, intense physical exertion, especially in someone who is usually sedentary.
A common example would be quickly shoveling snow after a storm in cold weather, an activity that can increase the risk of plaque rupture and trigger a coronary event.
Angina Pectoris
When an artery becomes narrowed by more than 60% due to plaque buildup, its ability to deliver oxygen to the heart can be compromised.
Angina pectoris occurs when the arteries cannot circulate enough bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood to supply the heart with adequate oxygen in certain areas.
Angina, the term used to describe the pain caused by a lack of oxygen to the heart, typically arises during physical exertion and quickly subsides with rest.
The Classic Form of Angina
The classic form of angina presents as chest pain radiating to the jaw and left arm.
However, it can also manifest in other ways, such as pain in the back, solely in the jaw, or only in the left arm.
Sometimes, Angina is Silent
Some individuals do not experience pain but instead feel a sudden shortness of breath during exertion, which is quickly relieved by rest. This phenomenon is known as “silent angina.”
Pain During Exertion, Relieved by Rest, and Reproducible
In all cases, pain occurring between the nose and the lower chest during exertion that dissipates with rest and reappears with similar efforts is a significant symptom. If you experience such symptoms, it is crucial to consult a doctor.
Stable angina, where symptoms remain consistent, is generally not life-threatening and can be treated in various ways.
Beware of Symptom Changes
However, any progression in symptoms—whether in intensity, frequency, or if they begin occurring at rest—is a sign of instability and could signal an impending heart attack. This means that damage could be occurring to the heart muscle.
It is crucial to seek medical attention promptly. If you have any concerns, do not hesitate to call 911!
No one is immune
No one is immune to coronary artery disease.
It’s important to remain vigilant, both for yourselves and those around us, by recognizing the signs, symptoms, and risk factors.
Some factors increase the risks
Certain factors increase the risk of developing coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease. Some are non-modifiable, such as being male, aging, and having a family history of the disease.
However, others can be influenced by lifestyle choices, such as smoking, high cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> levels, physical inactivity, diabetes, and high bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood pressure.
Investigation of Stable Angina
The investigation of stable angina aims to confirm the diagnosis, assess the severity of the underlying coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease, and establish an appropriate treatment plan.
Diagnosis is often based on the patient’s description of symptoms during their medical consultation.
Tests Ordered:
Electrocardiogram (ECG):
Although often normal in cases of stable angina, this is a basic test useful for evaluating the heart’s electrical activity.
Stress Test (Treadmill):
This test is commonly used to support the suspicion of coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease. It records the heart’s electrical activity during physical exertion, helping to detect electrical changes when there is a blockage in the heart’s bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow.
If a stress test is not possible or inconclusive, imaging tests may be used for a more thorough evaluation:
Stress Echocardiography
Myocardial Perfusion Imaging (MPI) under stress (or pharmacological stress using agents like Persantine or Dobutamine).
Coronary Angiography (Coronary Angiogram):
In cases where symptoms worsen, become more frequent, or occur at rest, a coronary angiography is often considered.
This procedure allows for direct visualization of the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that by injecting a contrast dye into the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood vessels, which is then revealed by X-rays. It is the gold standard test for identifying blockages or narrowing of the arteries.
A coronary CT scan may also be requested to provide a detailed view of the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that.
Treatment of Stable Angina
Medical guidelines generally recommend a conservative approach.
The treatment of stable angina involves a combination of medication therapies and lifestyle changes aimed at preventing cardiovascular events and managing symptoms.
- Medications:
Several types of medications work by reducing the oxygen demand of the heart muscle or by dilating the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that.
Antiplatelet agents (e.g., aspirin): These help prevent bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood clots from forming, reducing the risk of heart attack.
Statins: Cholesterol-lowering medications to reduce the risk of plaque buildup in the arteries.
- Lifestyle Changes:
In parallel, patients are encouraged to adopt healthier lifestyle habits in order to reduce their risk factors.
When symptoms can no longer be managed with pharmacological therapy or in cases of serious complications, more invasive interventions are considered:
Coronary angioplasty with stent placement: This procedure helps widen a blocked artery by inserting a stent to keep the vessel open.
Coronary bypass surgery: In more severe cases, bypass surgery is performed to create new pathways for bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow by bypassing the blocked arteries.
It’s important to note that coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease cannot be cured. The procedures described above are palliative treatments. The first involves compressing the cholesterolCholesterol is essential for the proper functioning of the human body, but it can also have harmful effects if present in excess. >> plaque, while the second creates bridges over the blockages.
Medical Follow-up
Regular follow-up is crucial for adjusting treatment, monitoring the progression of the disease, and preventing complications.
Prevention remains the best treatment
Prevention is the most effective way to combat coronary arteryThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that disease. Adopting healthy lifestyle habits, such as maintaining a balanced diet and engaging in regular physical activity, can significantly reduce the risks.