The mitral valve plays an essential role in bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow between the left atrium and the left ventricle. Far more than a simple membrane, it is a complex mechanical structure composed of a sturdy ring (annulus), two leaflets, chordae tendineae, and papillary muscles.
With each heartbeat, these components work in harmony to ensure a tight seal and prevent bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood from flowing backward.
This system can be compared to a sailboat: the annulus acts as the mast, the leaflets function like the sail, and the chordae, attached to the papillary muscles, keep everything properly tensioned and stable.
Proper mitral valve function depends on the integrity of all these components. If any one of them is altered, the balance of the entire system is disrupted.
Under normal conditions, this coordinated mechanism allows the valve to close effectively when the left ventricle contracts under high pressure.
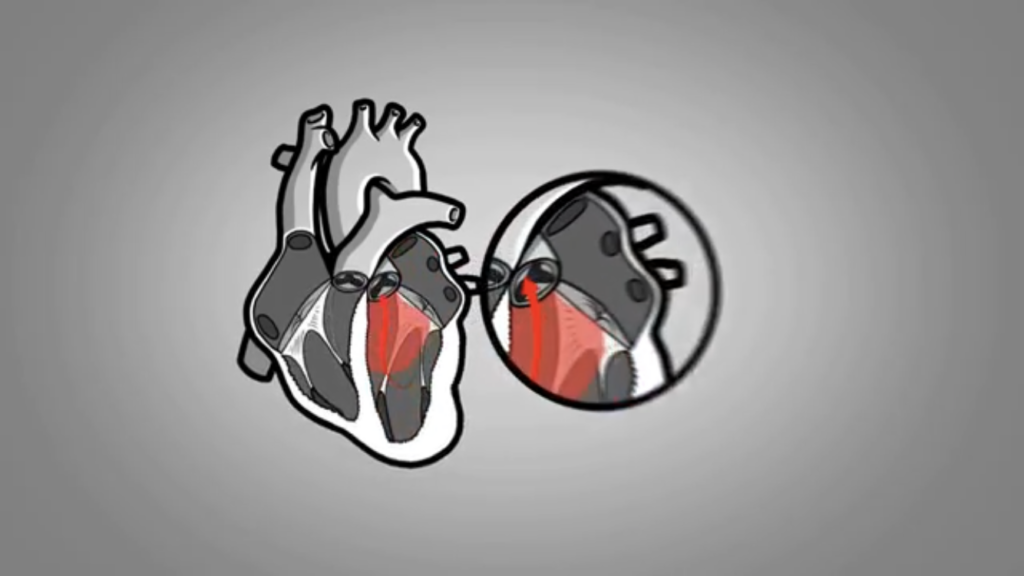
When one of the structures of the mitral apparatus no longer functions properly, closure becomes incomplete. An opening remains between the leaflets, allowing bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood to leak back into the left atrium—this is called mitral regurgitation.
This backward leak forces the heart to work harder, since part of the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood is circulating in the wrong direction.
or in a chronic form, when it appears gradually and progresses over time.
The chronic form is by far the most common type of mitral regurgitation. This article is entirely devoted to it.
Chronic Mitral Regurgitation
Chronic mitral regurgitation is the most common valvular heart disease in adults.
It results from a disorder of the mitral apparatus that develops and progresses slowly over time. This gradual evolution often allows the heart to adapt for a period before signs and symptoms appear.
Often Discovered by Chance
Mild mitral regurgitation usually causes no symptoms.
As a result, it is frequently discovered incidentally—either during a cardiac ultrasound performed for another reason or after a heart murmur is detected on physical examination.
Mitral valve prolapse is the most common cause of chronic mitral regurgitation. Although it usually remains stable and well tolerated, some forms may progress and lead to more significant leakage requiring specialized follow-up.
Other conditions can also gradually alter the mitral apparatus:
Damage to the papillary muscles after a myocardial infarction
Endocarditis, meaning a prior infection of the mitral valve
Left-sided heart failure that changes the shape of the ventricle
And, much more rarely today, sequelae of acute rheumatic fever
1- Consequence of a Myocardial Infarction
Among these causes, damage to a papillary muscle after a heart attack deserves special explanation. Even without rupture of the muscle, the healing process may slightly deform it or displace it from its normal position.
This shift creates abnormal tension on the chordae attached to that muscle. The tension is then transmitted to the corresponding mitral leaflet, which can no longer close properly against the other leaflet.
A small gap remains between them, allowing bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood to flow back into the left atrium—this is mitral regurgitation.
In this situation, the condition is referred to as “secondary” mitral regurgitation, because it is caused by disease of the heart muscle rather than a primary defect of the valve itself.
2- Infection of the Mitral Valve
Endocarditis, meaning infection of the mitral valve leaflets or chordae, is generally treated successfully with appropriate antibiotics.
However, even after the infection has resolved, scars or deformities may remain.
These residual changes reduce leaflet flexibility and mobility, which can compromise proper sealing and lead to leakage. The severity of this leak largely depends on the extent of damage caused by the initial infectious process.
3- Heart Failure
When the heart muscle weakens, as in heart failure, the left ventricle may enlarge and lose its normal shape.
This remodeling stretches the mitral annulus and displaces the papillary muscles, preventing the leaflets from closing properly. The valve becomes incompetent even though its structure was initially intact. This form is known as “functional” or “secondary” mitral regurgitation.
4- Acute Rheumatic Fever
Acute rheumatic fever, a complication of an inadequately treated streptococcal infection, can cause inflammation of the mitral valve.
Over time, this inflammatory process leads to thickening, stiffening, and sometimes partial fusion of the leaflets and chordae. The most common consequence is narrowing of the valve, known as mitral stenosis.
However, these same structural changes may also prevent complete closure, resulting in mitral regurgitation. It is not uncommon for both abnormalities to coexist.
Transient Mitral Regurgitation
A temporary lack of oxygen to a papillary muscle—such as during an episode of angina—can cause transient mitral regurgitation. This phenomenon is referred to as papillary muscle ischemia, sometimes called “papillary muscle angina.”
It is usually a reversible situation: the valve returns to normal function once bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood flow to the heart muscle is restored.
During physical exertion, marked shortness of breath—sometimes accompanied, sometimes not, by chest pain—may draw the attention of a healthcare professional.
Effects on the Left Ventricle
In chronic mitral regurgitation, part of the bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood ejected by the left ventricle flows back into the left atrium. This abnormal back-and-forth movement means that, from one heartbeat to the next, the ventricle receives an excess volume of bloodBlood is composed of red blood cells, white blood cells, platelets, and plasma. Red blood cells are responsible for transporting oxygen and carbon dioxide. White blood cells make up our immune defense system. Platelets contribute to blood.
To adapt to this additional load, it gradually enlarges.
The heart may compensate for this volume overload for many years, which explains why the condition can remain silent for a long time.
Over time, however, this persistent situation eventually leads to weakening of the heart muscle and more pronounced enlargement of the chamber.
The Chicken or the Egg?
As we have seen, chronic mitral regurgitation can lead to enlargement of the left ventricle.
However, the reverse is also possible: enlargement of this chamber can disrupt normal valve function and promote the development of leakage.
In practice, it is sometimes difficult to determine which phenomenon occurred first.
Highly Variable Symptoms
The manifestations of chronic mitral regurgitation are numerous and can vary greatly from one person to another.
Over the long term, significant leakage may gradually impair heart function. Even in the absence of noticeable symptoms, certain measurements obtained by echocardiography may justify corrective intervention.
The absence of symptoms does not mean the condition is harmless. Waiting for symptoms to appear may sometimes mean that the heart muscle has already sustained partially irreversible damage—hence the importance of regular medical follow-up.
Adapting to Evolving Knowledge
For many years, intervention was often delayed until symptoms appeared or indirect signs of worsening were observed.
Today, it is recognized that significant mitral regurgitation can lead to progressive damage to the heart muscle, even in the absence of marked symptoms.
When valve repair is considered highly likely to succeed and is performed in specialized centers, earlier intervention is now generally favored.
Treatment of Mitral Valve Regurgitation
When the decision is made to correct mitral leakage, three approaches may be considered:
Mitral valve repair (mitral valvuloplasty)
Mitral valve replacement
MitraClip
1- Mitral Valve Repair
Mitral valve repair is a surgical procedure that involves restoring the function of the affected valve rather than replacing it.
When feasible and performed by experienced teams, it provides excellent long-term results while preserving the natural valve.
By avoiding the implantation of a prosthetic valve, repair also helps prevent the constraints and potential complications associated with artificial valves, such as the need for long-term anticoagulation in certain cases or the risk of structural deterioration over time.
Read also: Mitral Valve Repair
2- Mitral Valve Replacement
When the valve is too severely damaged to allow durable repair, replacement becomes necessary. The procedure involves removing the diseased valve and replacing it with either a mechanical or biological prosthesis.
This approach effectively corrects the leakage but involves certain long-term considerations.
Mechanical valves are highly durable but require lifelong anticoagulation therapy. Biological prostheses, on the other hand, generally avoid prolonged anticoagulation, but their lifespan may be limited.
Read also: Mitral Valve Replacement
Surgical Approaches to the Mitral Valve
Mitral valve surgery can be performed using different approaches.
The traditional method involves a complete opening of the sternum, known as a sternotomy. This well-established technique provides excellent access to the heart and remains widely used.
In recent years, minimally invasive techniques have been developed, including procedures performed through a small incision on the right side of the chest. This approach allows access to the valve without fully opening the sternum.
When appropriate, minimally invasive surgery is generally associated with faster recovery, shorter hospitalization, less postoperative pain, and a more discreet cosmetic result.
The choice of technique depends on the valve anatomy, the individual’s overall health, and the expertise of the surgical team.
3- Options for Patients at High Surgical Risk
In some individuals, the risk associated with open-heart surgery may be considered too high due to advanced age, associated medical conditions, or overall frailty.
In such cases, percutaneous repair of the mitral valve using a device such as the MitraClip may be proposed. This procedure is performed through a catheter, without opening the chest.
Although it does not completely eliminate the leak, this technique often reduces its severity, relieves symptoms, decreases repeated hospitalizations for heart failure, and improves quality of life.
Also read:MitraClip
Additional Testing Before Surgery
When conventional mitral valve surgery is planned—whether mitral valve repair or valve replacement performed through an open-chest approach—a coronary angiography is generally carried out before the procedure.
This test evaluates the condition of the coronary arteriesThe two coronary arteries, the right and the left, form the blood network that supplies the heart with oxygen and nutrients. They are located directly on the surface of the heart and branch into smaller vessels that. If significant narrowings are identified, they can be treated during the same operation, thereby avoiding a second intervention at a later time.
The treatment of mitral regurgitation does not rely solely on medications or surgery. Lifestyle measures play a fundamental role.
Regular cardiovascular exercise adapted to the individual’s condition is recommended, along with smoking cessation, a balanced diet, and maintaining a healthy weight.
Good oral hygiene is also essential to reduce the risk of valve infection.
Depending on the clinical situation, salt restriction and, in some cases, fluid limitation may be necessary, particularly in the presence of heart failure.
When mitral regurgitation is secondary to weakened heart muscle function with reduced ejection fraction, the standard recommendations for this condition also apply.
Chronic mitral regurgitation is a progressive condition whose manifestations may remain subtle for many years.
Whenever feasible, mitral valve repair is now the preferred approach.
Because each situation is unique, treatment decisions are made in partnership with the individual, taking into account overall health, expectations, and the most appropriate available options.